

Research by Diane Alexander, economist, Federal Reserve Bank of Chicago, Janet Currie, Henry Putnam Professor of Economics and Public Affairs, Princeton University, and Molly Schnell, assistant professor of economics, Northwestern University
Summary by Lisa Camner McKay, economics writer
Retail clinics offer convenient, low-cost preventive health care and treatment for minor injury and illness. When a retail clinic opens, the rate of visits to the emergency room for these low-severity conditions declines for people who live in close proximity.
Every fall, as the days grow shorter and the air turns colder, another somber seasonal marker arrives: the flu. The Centers for Disease Control and Prevention estimates that in the winter of 2018–19, about 42 million people got sick from the flu, causing 647,000 hospitalizations and 61,000 deaths.1 These numbers would be lower if more adults heeded medical advice to obtain a flu shot, yet only about one-third of prime-aged adults do so.
Enter the retail clinic. Retail clinics arrived on the health care scene in the early 2000s as a convenient and affordable alternative to doctors’ offices, urgent care centers, and emergency rooms (ERs). Because they are usually in big box stores or pharmacies such as Walmart and CVS, retail clinics are conveniently located. And because they serve customers on a walk-in basis, they are convenient to access. Their services include basic primary care for minor illnesses and injuries, such as sore throats, bug bites, and minor burns, as well as preventive primary care, such as vaccines and diabetes glucose monitoring.
Providing these medical services—at convenient times and locations—may affect how many people end up in the ER for minor conditions. The ER is an expensive (and often inconvenient) place to access such treatment. Indeed, a recent study found that the prices in retail clinics are around 80% lower than ER prices for the same service.2 Retail clinics thus have the potential to not only expand medical services but to do so while saving money. But do they live up to this potential?
This question animates a recent research article by Diane Alexander, Janet Currie, and Molly Schnell.3 While ideally researchers assess how a population’s health changes when a retail clinic opens, such extensive health data is difficult to assemble. To gain traction on the impact of retail clinics, then, Alexander, Currie, and Schnell analyze how the numbers of ER visits for different categories of illness are affected by the presence of retail clinics in the state of New Jersey. They find that people who live within two miles of a retail clinic after it opens do indeed have fewer visits to the ER for the minor illnesses and injuries that retail clinics treat than do people who live farther away. Retail clinics also reduce ER visits for illnesses that can be prevented via appropriate primary care—most notably, visits for the flu decline by 13%. This suggests that retail clinics, with their low, transparent prices and convenient hours, make an important contribution to the health care landscape.
A theory of retail clinic usage
Before diving into the data, Alexander, Currie, and Schnell develop a theory as to how the presence of retail clinics affects the health care setting in which patients receive treatment. This theory provides concrete predictions that they then test with data. The authors assume that patients select a venue based on the severity of their condition and the cost of the treatment, making retail clinics best suited for low-severity conditions, doctors’ offices best suited for mid-severity conditions, and the ER best suited for high-severity conditions. The arrival of a retail clinic, then, will affect how many people visit the ER via two mechanisms: substitution and prevention.
First, the authors theorize that patients with low-severity, treatable conditions will substitute the emergency room for a retail clinic when a retail clinic is convenient. These conditions include minor illnesses and injuries that can be treated by a nurse practitioner or general medical practitioner, such as ear infections, eye infections, upper respiratory tract infections, sore throats, urinary tract infections, sprains, and strains. The authors call this class of condition “primary care treatable.” Because these conditions require treatment relatively quickly, these patients may end up in the ER if they can’t get a doctor’s appointment. If a retail clinic opens nearby, however, some of these patients should switch to the clinic because of its convenience and low cost. In particular, patients with the least-severe conditions in these categories should be more likely to switch venues, leaving the ER to handle fewer but more severe visits in the primary care treatable category.
Second, the authors theorize that ER visits will be prevented when a retail clinic opens because more people will receive preventive primary care. In this class of conditions, dubbed “emergent, preventable,” the authors focus on influenza and diabetes. These are illnesses that can be avoided or controlled in an outpatient setting if they are treated properly (with flu shots and glucose monitoring), but if they go untreated, they will land some patients in the ER. When a retail clinic opens, more people should receive preventive primary care, thus reducing the number of ER visits. However, the severity of the condition for people who nonetheless develop influenza or diabetes complications (whether or not they received preventive care) should not be affected. Figure 1 shows how use of the ER is affected by the availability of retail clinics and primary care doctors.
1. Where patients are treated
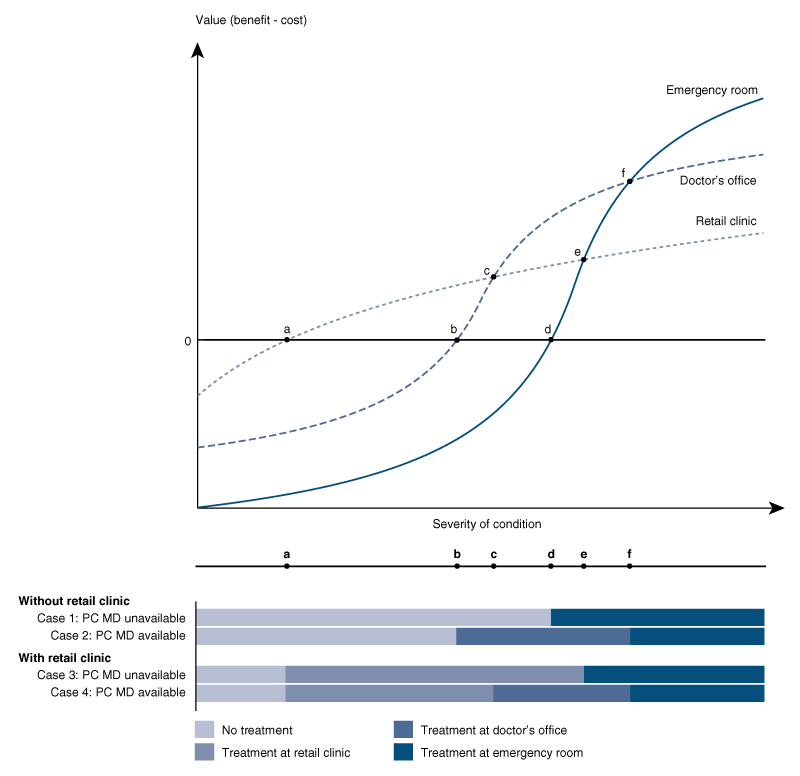
Source: Diane Alexander, Janet Currie, and Molly Schnell, 2019, “Check up before you check out: Retail clinics and emergency room use,” Journal of Public Economics, Vol. 178, October. Crossref
Retail clinics should not affect ER visits in all categories of illness or injury, however, as there are many conditions that clinics do not treat. These “emergent, non-preventable” conditions—e.g., poisoning, bone fractures, and childbirth—must be treated at an ER. And of course, the severity of the condition in patients treated at an ER should not be affected by the opening of a retail clinic.
Retail clinic zones
To test their theory, Alexander, Currie, and Schnell examine all 55 retail clinics in New Jersey that were open at some point between 2006 and 2014. Because the theory suggests that convenience is a key draw for retail clinics, they need to sort people into groups based on how convenient a retail clinic is for them. They do this based on address. People who live within a two-mile radius are viewed as potential patients of the clinic, while those who live two to five miles away are viewed as relatively unaffected by the presence of a retail clinic. (People who live more than five miles from a retail clinic are not included in the analysis because their health needs and outcomes are quite different from those who live closer to clinics, making them unsuitable for comparison.)
The authors then gather hospital discharge data from New Jersey’s uniform billing records, which include diagnosis codes (what patients were treated for), as well as the address of each patient. This allows the researchers to calculate the number of ER visits for their conditions of interest by patients who live 0–2 miles from a retail clinic (the treatment group) and by patients who live 2–5 miles from a retail clinic (the control group).
The data also include total “list charges” for each patient, which are the hospital’s charges for each billable treatment item the patient needed (this is not the amount that patients pay, as hospitals negotiate with insurers). The authors use total list charges as a measure for how severe the patient’s condition was. An influenza patient who was hospitalized will incur much higher list charges, for instance, than an influenza patient who simply needed fluids and then was discharged.
Of course, there is nothing magical about the two-mile mark from a retail clinic. Most likely, the use of a retail clinic gradually declines with distance. This means that some people who live three, four, and five miles away will use the retail clinic, too (although fewer will do so). Since Alexander, Currie, and Schnell include these individuals in their control group, their results will actually underestimate the real effect of a retail clinic.
Retail clinics reduce ER visits
The goal of the analysis is to compare the rate of ER visits (the number of visits in a week per 100,000 people) for each category of illness by residents who live 0–2 miles from a retail clinic with the rate of ER visits by residents who live 2–5 miles from a retail clinic. Before a clinic opens or after it closes, visits by the two groups follow similar trends. However, when a retail clinic is open, ER visits by the near group decline in every primary care treatable and emergent, preventable category that the authors analyze. Notably, the rate of visits for influenza falls by 13%, for sore throats by 12%, and for eye infections by 10%. Visits for the other primary care treatable ailments—urinary tract infections, upper respiratory infections, ear infections, sprains, and strains—all fall by about 6%. The last category, diabetes, sees the smallest effect, with a decline of 3%.
Importantly, the rate of ER visits by patients living near retail clinics does not fall for poisonings, bone fractures, or childbirth. If this rate did fall, it would suggest that there was some factor other than retail clinics that was affecting ER visits. The fact that it does not change adds confidence to the conclusion that it is the presence of retail clinics that is causing the decline in visits for the primary care treatable and emergent, preventable categories.
The authors also analyze the severity of ER visits when a retail clinic is open versus when it is not. Here too, the results affirm the theoretical predictions. The severity of ER visits in the primary care treatable category go up among people who live within two miles of an open retail clinic, suggesting that low-severity patients are the ones substituting retail clinics for ERs. No other illness category sees an increase in severity.
Better health, lower cost
These results suggest that improving access to primary care can reduce the number of patient visits at emergency rooms. This, in turn, should have real cost savings, as the ER is an expensive place to receive care. For this reason, it has been a long-standing goal of public health policy to reduce ER use for non-urgent care. Alexander, Currie, and Schnell show that convenient care—close to home, non-workday hours, transparent prices—offers a solution.
The authors estimate that the ER visits that did not occur because of retail clinics would have cost almost $800,000 per 100,000 people per year. If everyone in New Jersey lived within two miles of a retail clinic, this would result in an annual cost savings from reduced ER use of approximately $70 million. This number is based only on the conditions that the authors examine, thus the real number is likely even higher. While retail clinics could also increase costs by encouraging more primary care visits, at $100 per visit, it would take around 700,000 additional visits per year to retail clinics to offset the estimated savings from reduced ER use.
Notably, the bulk of these savings come from reductions in visits for influenza and diabetes. In other words, the cost savings are primarily the result of prevention, not substituting care at an ER for care at a retail clinic. A flu shot is far cheaper than hospitalization for influenza. While $70 million per year pales in comparison to overall health care spending in New Jersey, it is more than double annual state spending on community health centers and similar to the state’s share of Children’s Health Insurance Program expenditures.4
Beyond dollars and cents, this research indicates that retail clinics may improve health outcomes, a possibility that deserves further scrutiny. After all, flu season is here again.
Notes
1 Jamie Ducharme, 2019, “This past flu season was the longest in 10 years, the CDC says,” Time, June 20, available online.
2 Heidi Godman, 2016, “Retail health clinics: The pros and cons,” Harvard Health Blog, January 15, available online.
3 Diane Alexander, Janet Currie, and Molly Schnell, 2019, “Check up before you check out: Retail clinics and emergency room use,” Journal of Public Economics, Vol. 178, October. Crossref
4 For information regarding New Jersey’s spending on community health centers (federally qualified health centers) for FY2018, see State of New Jersey, Office of Management and Budget, 2017, The Governor’s FY 2018 Budget: Detailed Budget, report, Trenton, NJ, February 28, available online. Information regarding New Jersey’s share of CHIP spending for FY2017 is from the Medicaid and CHIP Payment and Access Commission, available online.






